When AI Can Listen in Real Time: What New Voice Models May Mean for Clinical Practice
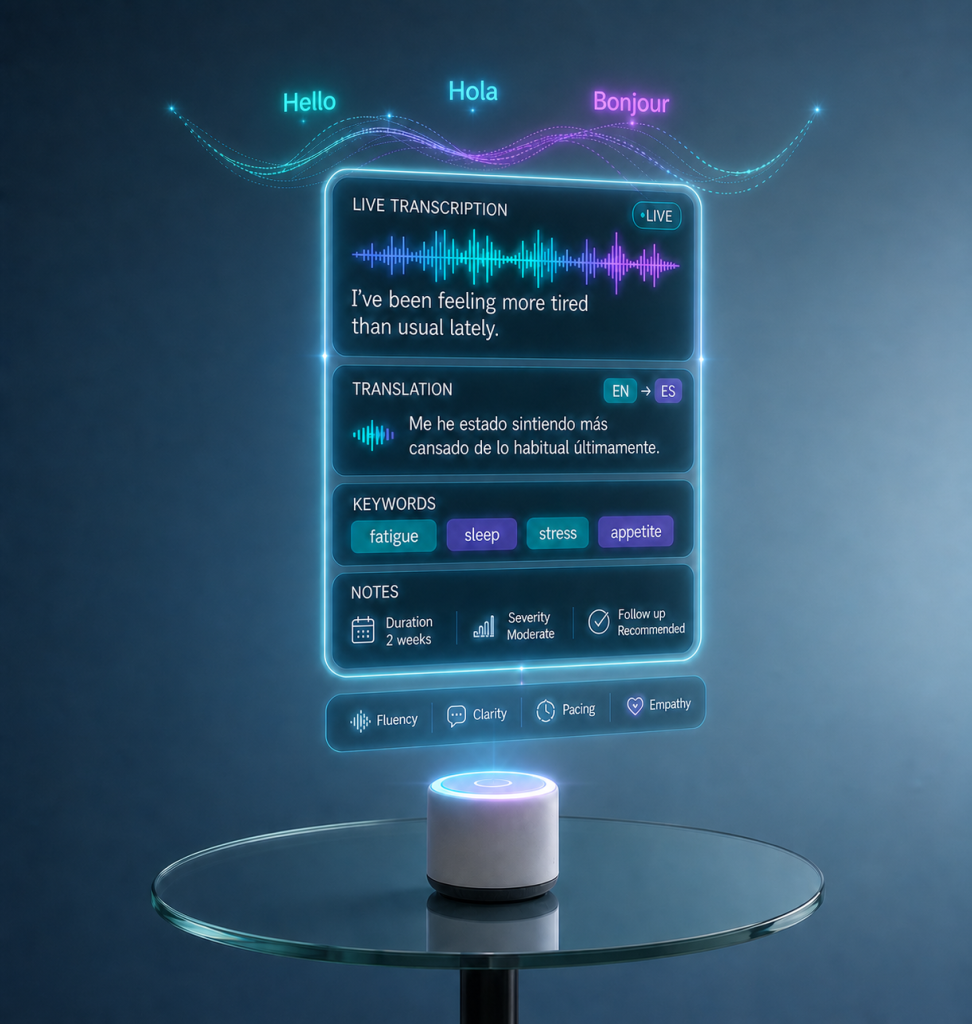
In many therapy settings, listening to a patient’s speech is a key part of understanding their needs. Therapists often record sessions, then spend time later writing notes or analyzing what was said. This process can be slow and sometimes separates the moment of listening from the moment of understanding. New voice-based AI tools are starting to change this by allowing speech to be processed and analyzed as it happens. OpenAI has introduced three new voice models that work in real time. GPT‑Realtime‑2 can hold more natural conversations and respond to more complex questions, using advanced reasoning. GPT‑Realtime‑Translate can translate speech from more than 70 languages into 13 languages while the person is still speaking. GPT‑Realtime‑Whisper can turn speech into written text immediately, without waiting for the speaker to finish. Together, these tools allow developers to create systems that listen, respond, and act during live conversations. For therapists, this may feel like a big change. Instead of only listening and then reflecting later, there is now the possibility of getting support during the session itself. For example, a system could help transcribe what a patient says, highlight important words, or track changes in speech over time. This may make documentation easier and reduce workload, especially in busy clinical environments. However, therapy is not only about words. It also includes tone, emotion, pauses, and the relationship between therapist and patient. While AI can detect some patterns in speech, it does not truly understand the person behind the words. This means that therapists still need to interpret meaning carefully and use their own clinical judgment. The translation model may be especially helpful when working with patients who speak different languages. It can support communication without always needing an interpreter. At the same time, language is complex and shaped by culture. Some meanings, emotions, or expressions may not translate perfectly. Therapists should remain cautious and check understanding when needed. From a practical point of view, these tools can support assessment and intervention. For example, a therapist could notice changes in fluency or word use more quickly. This may help in adjusting treatment plans earlier. It can also support patients practicing at home, especially if feedback is available in real time. At the same time, there are limits. AI systems are trained on large datasets, but they do not include every accent, dialect, or communication style. This means mistakes can happen. The system may misunderstand speech or give suggestions that do not fit the clinical situation. It is important not to rely on these tools without questioning them. For therapists who are still developing their skills, there is a risk of trusting AI too much because it sounds confident. However, good clinical reasoning takes time to build. AI should be used as a support tool, not as a replacement for thinking. Asking questions and reflecting on each case remain essential parts of practice. There are also ethical responsibilities. Patients should know when AI is being used and how their data are handled. Therapists must protect confidentiality and be aware that AI systems can include bias. In the end, the clinician is responsible for decisions, not the technology. Today, your data is like your fingerprint, unique and personal. If your data is used to train AI models, your voice, images, or other personal information could potentially be reused in different forms of content generation. This makes it essential to be careful when choosing which tools to use in clinical settings. Therapists should always check where data is stored, how it is used, and whether it is properly protected. Choosing platforms that prioritize privacy and confidentiality is not optional, it is part of ethical care. Clear consent, secure systems, and informed decision-making should guide the use of any AI tool in practice. Looking ahead, these voice models may become useful tools in everyday practice if used carefully. They can save time and offer helpful insights, but they do not replace human understanding. The role of the therapist remains central. Good care will continue to depend on a balance between using new tools and maintaining strong clinical judgment.